Strength Training for Bone Density
Why you don’t necessarily have to “LIFTMOR”

Peri-menopausal and post-menopausal women are being inundated with this message that they HAVE to perform heavy compound lifts to protect their bones.
If you listen to any “healthy aging” podcast, the message will probably be the same:
The ONLY way to stave off osteoporosis is by performing Deadlifts and Back Squats at 85% of your 1 Rep Max (1RM).
While I think this absolutely IS an effective way to improve bone mineral density (BMD), I DON’T think it’s the ONLY way.
Moderate intensity lifting can also be effective!
**To be clear, in this post I’ll be talking about high, moderate, and low intensity weight training. In this context, intensity is always referring to percentage of 1 Rep Max. Typically high intensity is around 85% of 1RM, moderate intensity is around 50-75% of 1RM, and low intensity is less than 50% of 1RM - but the exact breakdown will depend on the study.
So buckle up, because we’re about to do a deep dive in the research!
First off, where do we get this recommendation that we HAVE to do compound lifts at 85% of our 1RM?
A study with a catchy name swept the scene in 2018: it’s the LIFTMOR randomized control trial. Anytime I even MENTION bone density on Instagram, I get an onslaught of comments about the LIFTMOR trial.
They almost always go something like this:

The general understanding (from this commenter and many others) is that while we might be able to improve MUSCLE by lifting light to moderate loads, this is NOT true for bone. Improving bone health REQUIRES heavier loads - and the conclusion is always that the LIFTMOR trial is what proves this. (Spoiler Alert- This isn’t what the research says)
So let’s look at the LIFTMOR study!
The Experimental Group did a warm-up at 50-70% of their 1RM, and then followed it by 5 sets of 5 reps at 85% of their 1RM for the following movements:
Deadlifts
Back Squats
Overhead Presses
The experimental group ALSO did impact loading via “drop landings” where they held onto a bar overhead, and then intentionally landed heavily for max impact.
On the other hand, the Control Group did walking, low intensity exercises (calf raises, lunges, shrugs, standing forward raises), and stretching. The researchers state that the Control Group protocol was “designed to improve balance and mobility but provide minimal stimulus to bone.” This group ended the study lifting a total of only 3 kg (or 6.6 lbs).
The study results? The group that did heavy lifting (Experimental Group) showed a 2.9% increase in Lumbar Spine BMD and a 0.3% increase in Femoral Neck BMD.
And it comes at NO surprise that the Control Group did NOT show improvements in BMD, because they specifically designed their workout to “provide minimal stimulus to bone.”
So while the LIFTMOR trial is GREAT, and it DOES show the benefits of compound heavy lifting, it does NOT disprove (or make ANY claim) about lifting at moderate intensities (65-80% of 1RM) to muscle fatigue.
I think it’s also important to note that they didn’t ONLY perform heavy lifting. They also included fairly intense impact training through the “drop landing” exercises. So it’s impossible to say that the changes in BMD were from the resistance training alone.
I want to reiterate that I am absolutely a fan of the LIFTMOR trial. It’s a really well-designed study, and I think it shows the effectiveness of heavy, compound lifts. I just don’t think we can use this study to say that moderate lifting or other modalities AREN’T effective.
We need to look at research COMPARING moderate & heavy intensity lifting and their effects on bone density.
The first study I want to show you is this systematic review and meta analysis from Souza et al. in 2020 titled “High and low-load resistance training produce similar effects on bone mineral density of middle-aged and older people”
They point out in this study that “it is generally recommended that aging individuals should perform Resistance Training using higher loads (≥70% 1RM)… However, since these studies compared training with non-exercise or usual care controls, it is difficult to determine if high-load Resistance Training presents greater effectiveness than low-load.” - aka: they’re mostly designed similarly to the LIFTMOR trial, where the control group is minimally loaded.
So what did they do? They looked at 6 different randomized clinical and controlled trials to compare the effects of moderate intensity lifting (which they define as training at less than 70% of 1RM) and high intensity lifting (training above 70% of their 1RM) on bone mineral density.
They concluded from these studies that “both high- and low-load Resistance Training protocols provide similar effects in BMD, which suggests that the intensity threshold to provide adaptations might be as low as 40% of 1RM, as long as effort is adequate.” ** (We’re going to touch on this effort piece in a bit, so stay with me)
Let’s look at another one:
I present to you this systematic review and meta analysis from Kistler-Fischbacher et al in 2021 titled “The effect of exercise intensity on bone in postmenopausal women.”
This analysis compared 100 different research studies (yup… way more than 6) and compared low, moderate, and high intensity training. Here was how they defined the resistance training:

Table 1 from Kistler-Fischbacher, M., Weeks, B. K., & Beck, B. R. (2021). The effect of exercise intensity on bone in postmenopausal women (part 1): a systematic review. Bone, 143, 115696.
So the LIFTMOR trial would fall under that “high intensity" category because they lifted at 85% of their 1RM, and how I personally train would fall in the “moderate intensity” category, working around 65-80% of my 1RM (**I’ll make a comment on the rep scheme later, when we address the “effort” piece… )
What did their data show?
Bone density was IMPROVED in ALL categories: low, moderate, AND high intensity.
Let’s look at the Femoral Neck BMD measures:
The bold black diamond is representing the summation of all the data for that category, and in each category you can see that the diamond is shifted so that it favors the exercise group over the control. In fact, the high intensity group was the least favorable for the Femoral Neck BMD.
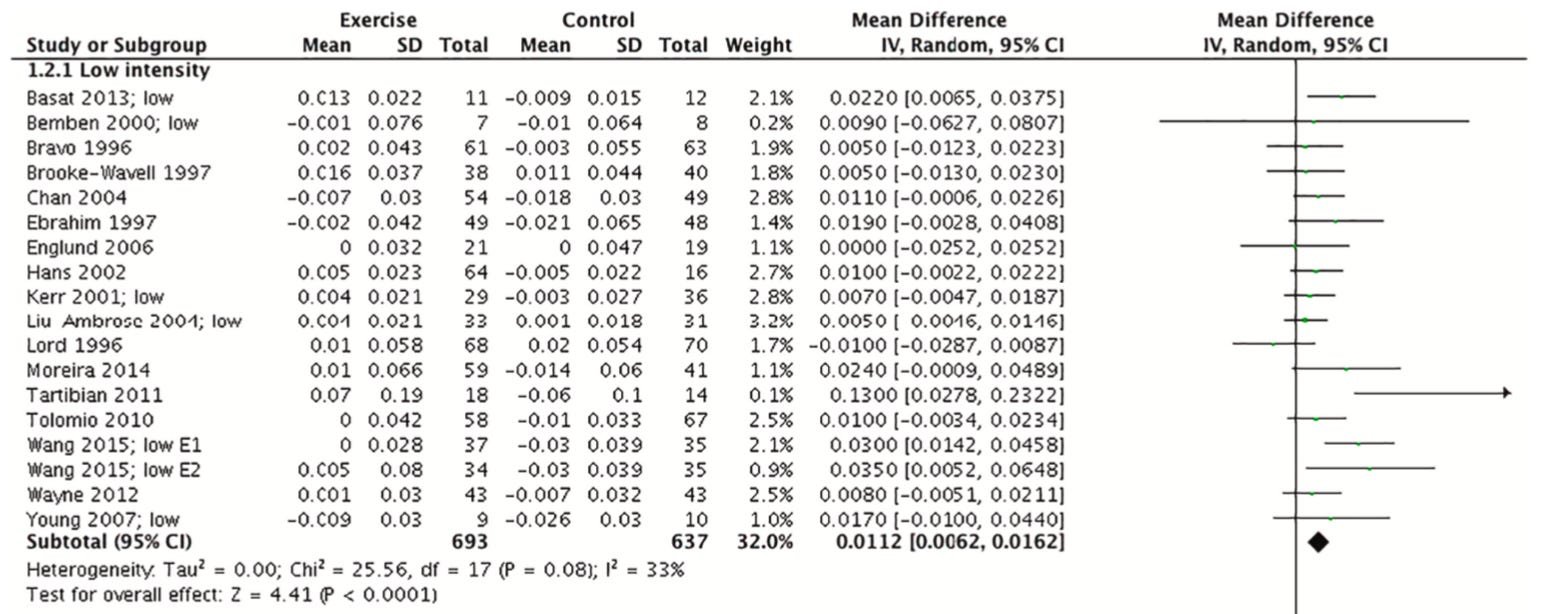
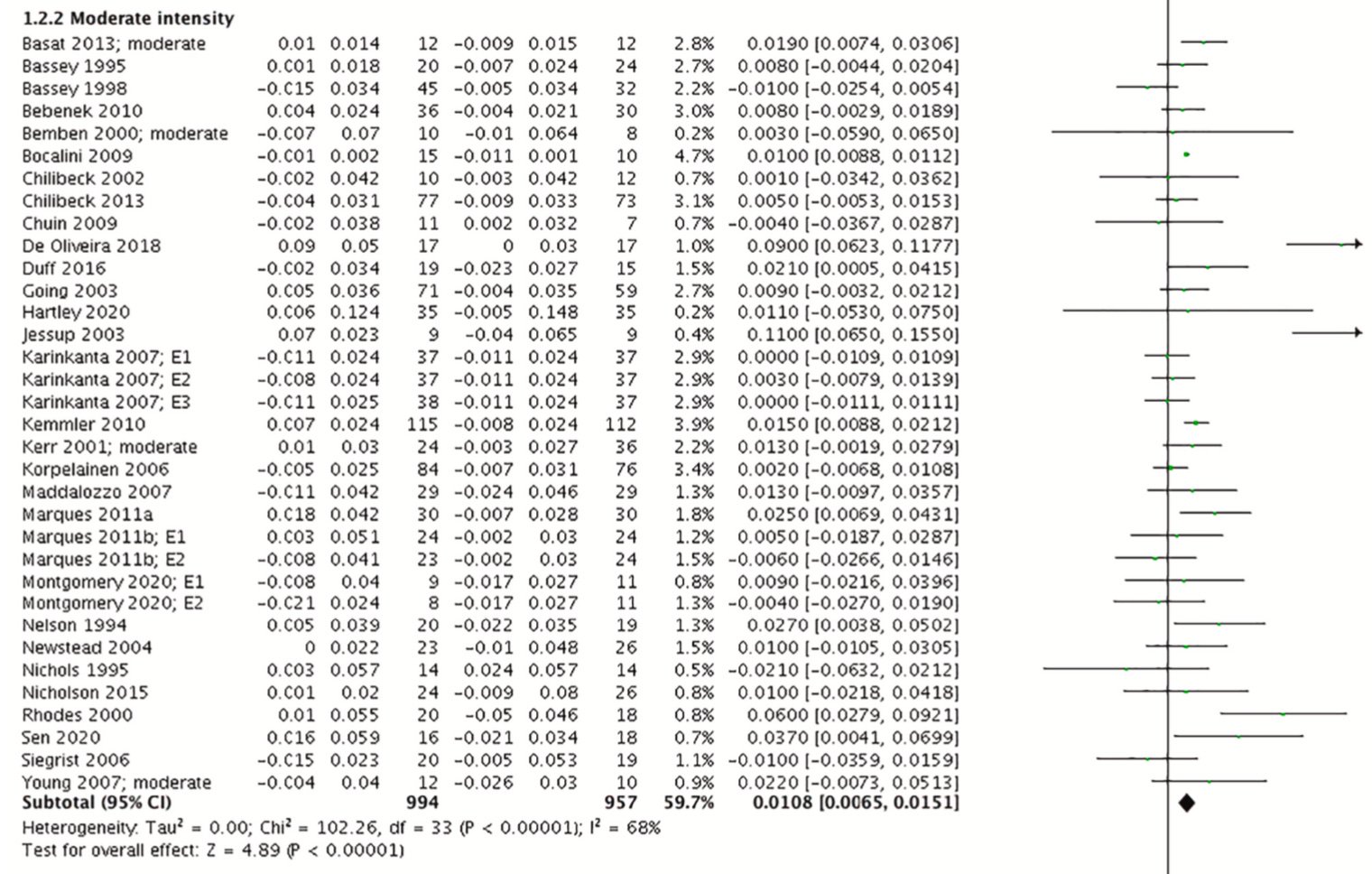
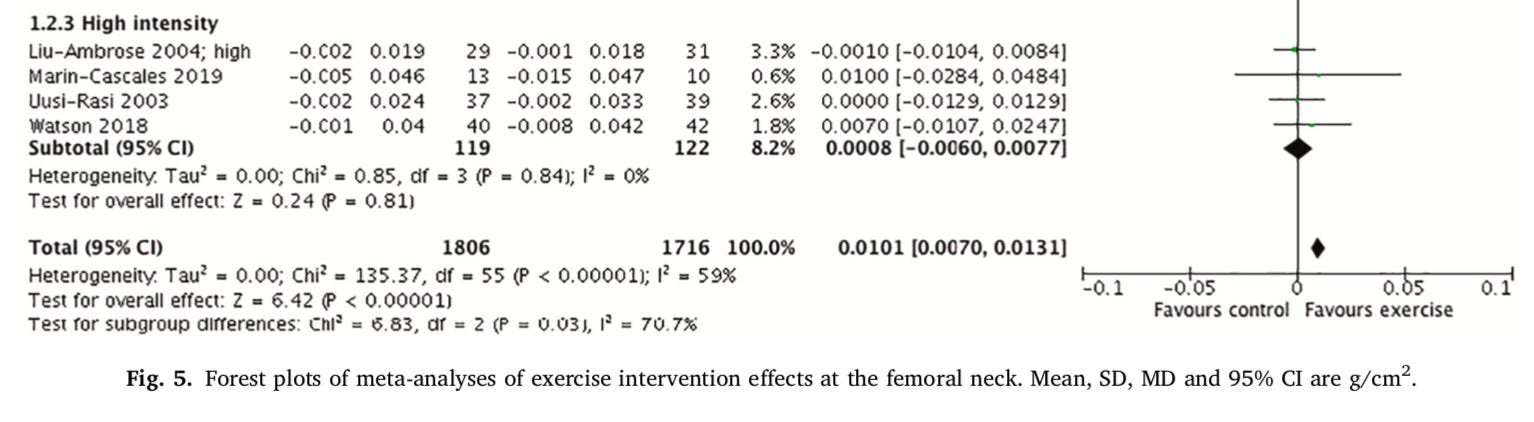
Figure 5 from Kistler-Fischbacher, M., Weeks, B. K., & Beck, B. R. (2021). The effect of exercise intensity on bone in postmenopausal women (part 2): a meta-analysis. Bone, 143, 115697.
I’ll spare you more screenshots from the data, but this study also demonstrated improvements in Lumbar Spine BMD for all 3 intensity categories, and favored moderate intensity training for Total Hip BMD.
In their conclusion, the authors state, “the optimal exercise prescription for postmenopausal bone health in healthy individual should include moderate to high intensity progressive resistance training alone or in combination with weight bearing impact training.”
So after looking at 100 different studies, we see that BOTH moderate AND high intensity was effective at improving BMD. (and even some low intensity!)
7 Additional Considerations (because there’s always nuance):
1. Effort Matters
Many of the studies that compare high and low intensity training try to match “training volume” - so for example, in this study by Bemben & Bemben, they had the High Intensity training group lift at 80% of their 1RM and perform 3 sets of 8 reps, and they had the Low Intensity training group lift 40% of their 1RM for 3 sets of 16 reps.
While I can understand the logic from a “training volume” standpoint (if you’re training at half the intensity, then you’d double the reps), this is actually really different from an EFFORT standpoint.
Here’s what I mean.
If you’re familiar with the Holten Diagram (shown below), then lifting at 80% of your 1RM typically means you can do about 11 reps before hitting muscle failure.
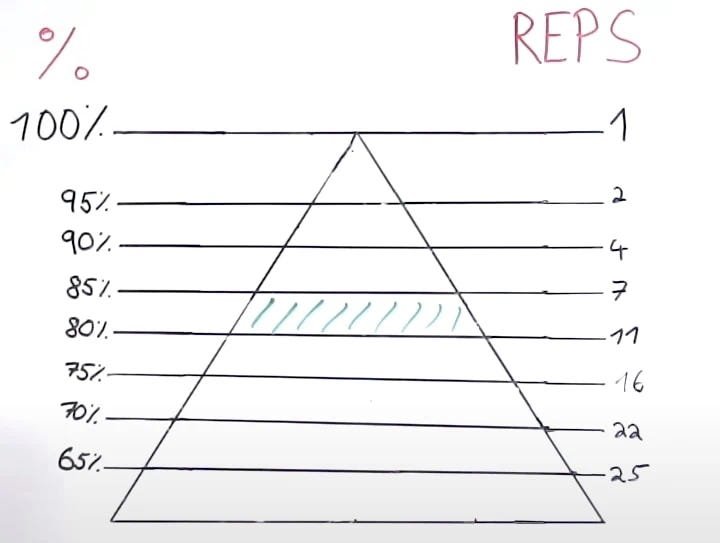
Image from physiotutors.com
And if you’re training at 40% of your 1RM, then you can do 30+ reps before hitting muscle failure…(40% of your 1RM isn’t even shown on this chart, but you can see what I mean…)
Why does this matter? Well when a study simply doubles the reps, it doesn’t take into account EFFORT. It doesn’t factor into the equation that this relationship between “% of your 1 Rep Max” and “Reps to Muscle Failure” isn’t linear!
Someone training at 40% of their 1 Rep Max and only doing 16 reps has MANY more reps in the tank before hitting muscle failure.
This is why I don’t like to necessarily go by reps, but instead, I encourage people to choose weights and work to muscle fatigue (meaning just several reps away from failure). This ensures that the EFFORT remains high, no matter what weight they’re using!
I think it’s also important to note that this Bemben & Bemben study STILL showed improvements in bone density for the group that was only lifting 40% of their 1RM and not getting close to muscle failure. Here are their results:

Figure 1 from Bemben, D. A., & Bemben, M. G. (2011). Dose–response effect of 40 weeks of resistance training on bone mineral density in older adults. Osteoporosis international, 22, 179-186.
You can see by this chart, that High Intensity (80% of 1RM) showed better improvements for Spine BMD, but actually Low Intensity (40% of 1RM) showed better improvements for Femoral Neck BMD.
Still, when in doubt, I like effort to remain high, and I encourage people to work close to muscle failure since we see this as being an important factor for muscle strength.
2. The Presence of Muscle Mass is Protective to Bone
One of the most interesting things I’ve read while researching for this post is that the actual PRESENCE of muscle tissue is protective to bone tissue.
Simply put, having muscle mass is good for your bones!
No, I’m NOT just saying that if you lift weights, the effect of lifting is good for both muscles and bones. I’m literally saying that the muscle tissue ITSELF plays a role in bone health.
Muscle tissue can communicate to bone through the release of Myokines, which are modulated by exercise. These Myokines have the ability to positively influence bone formation. Resistance training INHIBITS a Myokine called Myostatin, which is involved in the formation of osteoclasts and the breaking down of bone tissue.
Quoting Souza et al. (2020), “Previous studies showed that muscle tissue seems to influence bone health and factors produced by muscle contractions, such as myokines, might also contribute to bone formation. Considering that these factors might be influenced by different loading conditions, these evidences suggest that triggers for bone synthesis involve more than only mechanical factors; therefore, the load threshold for inducing osteogenic response may be smaller than previously thought.”
Since we KNOW that we can improve muscle mass with many different loading intensities and frequencies, (check out this meta analysis if you don’t believe me) then it makes sense to conclude that this protective effect of muscle to bone doesn’t require lifting at 85% of your 1RM.
3. “Segmented Sets” Can Make Lifting at Higher Intensities More Accessible
While obviously after all this I’m not saying you HAVE to lift at 85% of your 1RM, I do want to offer a suggestion to Loa Movement members (and at-home weight lifters) that can help include some higher intensity lifts.
You’ve probably heard of the concept of “drop sets'“ - where you lift a heavy weight to your max, and then drop the weight and grab a lighter set and lift to your max again.
Well I’m taking this concept and re-coining it as Segmented Sets.
Here’s Why: In Loa Movement classes we often use 1 minute sets, meaning for some sets we don’t count our reps, but rather we choose a weight and attempt to work close to muscle failure within 1 minute. (You can read why we do this HERE).
I’ve had members say in the past “I feel like I want to go up in weight for this movement, but I can’t make it the full minute.” Enter Segmented Sets.
Start off the minute with a heavy weight and go as long as you can, and then when you can’t go anymore, grab a lighter weight to finish the minute.
I actually see this concept used in a study by Holubiac at el. where they made the participants perform 6 reps at 70% of 1RM and then immediately 6 reps at 50% of their 1RM. At the end of the study, participants saw a 1.8% increase in Lumbar Spine BMD.
I actually just did this today when I was teaching Lower Body - I started my Rear Foot Elevated Split Squat holding 30 lbs, and when my body couldn’t continue, I quickly swapped it out for a 20 lb dumbbell. This meant I was getting the stimulus at lifting around 80% of my 1RM, and then finishing the minute at a lower intensity.
Again, I don’t think this is REQUIRED, but I do think it’s a fun way to challenge yourself, keep effort high, and add in some higher intensity lifts.
4. Weighted Vests Can Be A Good Thing, But Beware of Trade-offs
I feel like I couldn’t write this post and NOT include SOMETHING about weighted vests. This seems to be all the rage for influencers in peri-menopause… or at least that’s what my Instagram algorithm is making me believe!
I wasn’t able to find a solid study that JUST looked at the use of weighted vests. Most studies combined weighted vest walking with some other modality (like weight training or jumping).
For example, the study by Jessup at al. had participants weightlifting at 50-70% of their 1RM and wearing a weighted vest for walks. They started the weighted vests light, but worked up to 10% of bodyweight by the end of the study. Participants saw an unexpectedly LARGE increase in BMD (11% increase… which is around 4x more than the LIFTMOR trial).
Another study by Snow et al. combined walking with a weighted vest and jump training. While this study only had 18 participants (9 in experimental group and 9 in control) they did conduct the study over the course of 5 years and found improvements in hip BMD.
Overall, the research does seem suggestive that supplementing your training with walking using a weighted vest (around 10% of your bodyweight) may have a positive influence on bone density, BUT, it’s always important to weigh the trade-offs.
Here’s what I mean: If walking with a weighted vest leaves your back sore or your knees hurting, it’s probably NOT worth it! This will inevitably affect your ability to be consistent with your workouts.
We also don’t know how wearing a weighted vest will affect your walking mechanics: such as arm swing or ribcage expansion.
So my advice concerning weighted vests: Try it out (if you want)! If it doesn’t give you pain, it could be a good option, but also it’s not REQUIRED to improve bone density.
5. Fueling Matters (Both macro and micro nutrients)
I’m not going to go in detail here because nutrition is NOT my speciality, but I do think it’s important to occasionally zoom out and look at the body as a whole.
Obviously exercise is not the ONLY thing that influences bone density.
When women train in a state of Low Energy Availability (aka: inadequate caloric intake to fuel their training), it is detrimental to their bone health.
I think this is very person-dependent (based on genetics, activity levels, etc), and I’d recommend working with a dietician if this is something you need more guidance around.
When it comes to micronutrients, we know that calcium and vitamin D are incredibly important for our bones! Supplementation may be the correct route, but I’m also always going to advocate for getting it the old-fashioned way: outside! We need sunshine!
6. Multimodal Exercise Might Be More Effective
What do I mean by “multimodal?” Including a variety of forms of movement in your life!
You’ll notice that studies looking at bone density often include more than JUST weight training.
For example, the LIFTMOR trial did “drop training” for impact. Many studies include jumping, weighted-vest walking, or even dancing!
If you’re new to exercise, first and foremost I would prioritize resistance training. Lifting weights definitely seems to be the most beneficial in terms of longevity across the board.
But, if you’re already in a routine of lifting, consider adding other forms of movements! Especially movement that provides some impact, such as: jumping (if you’re a Loa Member, take our BURST classes!), playing tennis, walking, jumping rope, hiking, or dancing.
Movement is medicine!
7. Consistency is Key
Want to know something that I think is WILDLY overlooked in exercise? ENJOYMENT.
If you enjoy your workouts, you’re going to be more consistent. Plain and simple.
And consistency REALLY REALLY matters.
In order to make necessary changes at the bone, we really need to be training around 2-3x per week… for life.
We see that when training stops, bone density will decline back to baseline, so a routine that allows you to be consistent is absolutely key for lasting change.
Pain and injury also play a major role in consistency.
For me personally, I loved CrossFit style workouts and barbell movements (similar to what you see in the LIFTMOR trial), but my body didn’t love it…
I was constantly dealing with back injuries, knee injuries… you name it! (And this was in my 20’s! When I was supposed to be pain-free and loving life!)
These days, I do more isolated movements using dumbbells, working around 60-70% of my 1RM. (aka: I teach classes for Loa Movement 4-5 days a week!) And you know what? I feel a million times better. I can actually go on walks, hike, and do MORE activities that I love.
So if you’re someone that feels like your workouts are limiting the rest of your life, I urge you to find a way to workout that allows you to do MORE, not less.
I’d rather “do more” than LIFTMOR ;)
Now I understand some people CAN do barbell movements at 85% of their 1RM and be just fine, and that’s great too! No need to change. I just hope you read this and realize that’s not the ONLY way to improve bone density.
In conclusion, lifting at high intensity is effective for improving bone density, BUT, so is lifting with high effort at lower intensities!
Find a plan that you enjoy, where you can put in high effort and be consistent.
This is why I try to design every Loa class based on the 3 E’s: effective, efficient, and enjoyable - because that’s what allows me to show up week in, week out.
You can workout with me for 7 days free- just click HERE!
Sources:
Watson, S. L., Weeks, B. K., Weis, L. J., Harding, A. T., Horan, S. A., & Beck, B. R. (2018). High‐intensity resistance and impact training improves bone mineral density and physical function in postmenopausal women with osteopenia and osteoporosis: the LIFTMOR randomized controlled trial. Journal of Bone and Mineral Research, 33(2), 211-220.
Souza, D., Barbalho, M., Ramirez-Campillo, R., Martins, W., & Gentil, P. (2020). High and low-load resistance training produce similar effects on bone mineral density of middle-aged and older people: a systematic review with meta-analysis of randomized clinical trials. Experimental gerontology, 138, 110973.
Kistler-Fischbacher, M., Weeks, B. K., & Beck, B. R. (2021). The effect of exercise intensity on bone in postmenopausal women (part 1): a systematic review. Bone, 143, 115696.
Kistler-Fischbacher, M., Weeks, B. K., & Beck, B. R. (2021). The effect of exercise intensity on bone in postmenopausal women (part 2): a meta-analysis. Bone, 143, 115697.
Bemben, D. A., & Bemben, M. G. (2011). Dose–response effect of 40 weeks of resistance training on bone mineral density in older adults. Osteoporosis international, 22, 179-186.
Weakley, J., Schoenfeld, B. J., Ljungberg, J., Halson, S. L., & Phillips, S. M. (2023). Physiological responses and adaptations to lower load resistance training: Implications for health and performance. Sports medicine-open, 9(1), 28.
Kirk, B., Feehan, J., Lombardi, G., & Duque, G. (2020). Muscle, bone, and fat crosstalk: the biological role of myokines, osteokines, and adipokines. Current osteoporosis reports, 18(4), 388-400.
Currier, B. S., Mcleod, J. C., Banfield, L., Beyene, J., Welton, N. J., D'Souza, A. C., ... & Phillips, S. M. (2023). Resistance training prescription for muscle strength and hypertrophy in healthy adults: a systematic review and Bayesian network meta-analysis. British Journal of Sports Medicine, 57(18), 1211-1220.
Holubiac, I. Ș., Leuciuc, F. V., Crăciun, D. M., & Dobrescu, T. (2022). Effect of strength training protocol on bone mineral density for postmenopausal women with osteopenia/osteoporosis assessed by dual-energy X-ray absorptiometry (DEXA). Sensors, 22(5), 1904.
Jessup, J. V., Horne, C., Vishen, R. K., & Wheeler, D. (2003). Effects of exercise on bone density, balance, and self-efficacy in older women. Biological Research for nursing, 4(3), 171-180.
Snow, C. M., Shaw, J. M., Winters, K. M., & Witzke, K. A. (2000). Long-term exercise using weighted vests prevents hip bone loss in postmenopausal women. The journals of gerontology. Series A, Biological sciences and medical sciences, 55(9), M489–M491. https://doi.org/10.1093/gerona/55.9.m489
De Souza, M. J., West, S. L., Jamal, S. A., Hawker, G. A., Gundberg, C. M., & Williams, N. I. (2008). The presence of both an energy deficiency and estrogen deficiency exacerbate alterations of bone metabolism in exercising women. Bone, 43(1), 140-148.
Huovinen, V., Ivaska, K. K., Kiviranta, R., Bucci, M., Lipponen, H., Sandboge, S., ... & Nuutila, P. (2016). Bone mineral density is increased after a 16-week resistance training intervention in elderly women with decreased muscle strength. European journal of endocrinology, 175(6), 571-582.